Clinical Course for Daniel Katz-Stein, Anaplastic Oligodendroglioma
February
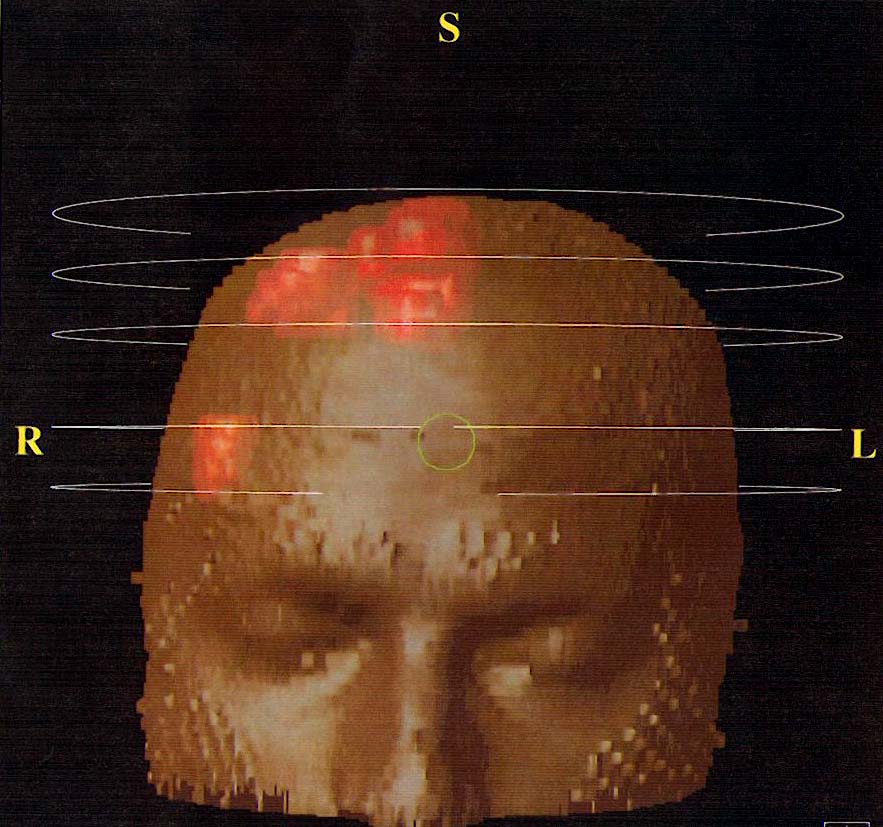
1995: New
onset seizure X 2, gran mal.
MRI demonstrated a 2.5 mm by 5mm mass lesion in the
right frontal area, just anterior to the motor cortex.
He was given dexamethasone 5 mg q6h, and dilantin and
referred for surgery.
March
1995: Complete surgical resection of tumor, by surgeon
Joseph Goodman,
Arthur James Cancer Research Center
,
Ohio
State University. Pathology
reported grade 1 oligodendroglioma, with all tumor margins
visualized. No
adjuvant therapy. Recovery
from surgery was uneventful.
July
1996: 4 grand mal seizures in 4 hours. He was referred
to a neurologist for follow up.
Seizures were diminished with medicine, but were not
completely controlled. He
experienced partial complex seizures either daily or weekly.
July
1999: New
tumor growth demonstrated on annual MRI.
September
1999: Complete
surgical resection of tumor by Peter M. Black, Brigham and
Women’s Hospital,
Harvard
University
. Pathology
reported of a grade2 oligodendroglioma.
Other pathological features of this tumor included a
MIB labeling ratio of 8 %, infiltrating into healthy brain
tissue, but was not anaplastic.
Full resection of tumor required excision of a
portion of the supplemental motor area.
Recovery was complicated by dense left sided
hemiparesis and abscess at surgical site. Hemiparesis
resolved to about 80% of pre-surgical function within the
first year.
October
1999: Abscess
evacuated with port placed to drain infection.
Cultures grew P. acnes.
Hospital stay of 21 days included IV PCN G, drain of
infection every other day with intraport injection of
vancomycin, 2 additional surgeries for port replacement.
IV continued for 6 weeks total.
Port removed in April 2000.
September
2000 – August 2002: 2 years of remission after the
second surgery. He
did not have seizures, was able to drive and work 70 % FTE.
August
2002: Myoclonic seizure, with Jacksonian march (foot
through leg, upper body and arm) and Todd’s postictal
paralysis. August
MRI demonstrated no obvious pathology.
Seizures continued weekly, then daily, then multiple
daily. November
MRI demonstrated 3.5 cm parafacine mass, enhanced with
Gadolinium. PET
demonstrated enhancement with glucose and methionine,
indicating high grade malingnancy.
December
2002: Complete
resection of tumor by Black.
Pathology reported anaplastic oligdendroglioma, rare
astrocyte involvement, +vascular proliveration, minute foci
of necrosis, foci of brisk mitoses, MIB1 varies from region
to region, 30% – 50%.
January
2003: Status
epilepticus – 10 – 15 minute complex partial seizures
with 5 to 10 minutes in between for 4 hours.
CT and MRI indicated CSF with high protein density,
and infection could not be excluded.
January
2003: Infection
site evacuated. Gross
infection found in dura, skull fragment and surgical cavity.
Cultures showed methicillin sensitive S. aureus
and P. acnes.
Further treatment included 8 weeks IV vancomycin and
rocephin and 2 weeks oral duracef.
February MRI, although obscured by motion artifact
from seizure activity, showed improvement from January
postoperative MRI.
April
2003: MRI
demonstrated 3 cm parafalcine mass that gad enhanced, with
some ring enhancement. April
MRI read by one neuroradiologist as “consistent with
recurrent abscess” and another neuroradiologist as
“recurrent tumor”. Treatment
presumed abscess and IV started with maxipime and
metrodinozole.
May
2003: MRI
demonstrated parafalcine mass and cortical mass, enhancement
consistent with tumor. Black
recommends radiation, Weinstein clears for adjuvant therapy
(chemo or radiation).
May/June/July
2003: CCF team decides surgery is not an option,
composite MRI/PET/CT demonstrates multiple lesions,
recurrent and malignant.
Final recommendation is IMRT radiation (31
treatments) with concurrent (42 days) Temodar chemotherapy
plus 6 months additional chemotherapy.
Jan
2004: After 4 courses of Temodar chemotherapy (5
days on/23 off), MRI is still 'stable,' but starts to
experience mini-seizures in his left leg. His ability
to walk decreases from mile to .2 of a mile in two
months. He experiences serve headaches.
Mar
2004: After 6 courses of Temodar chemotherapy, MRI
shows still stable. His headaches have reduced
by increasing Zonegran, but clinical symptoms remain.
Decide to change to change course of Temodar chemotherapy
to 1/2 strengeth - 6 weeks on/ 2 weeks off.
{kind=link}